It’s very common for people who have an eating disorder to identify as a highly sensitive person (HSP). While it may sound like a made-up term, this is actually a scientifically studied genetic condition. One of the notable traits is that HSPs are often more sensitive to food and eating. They may have significant differences in how they experience food and sensations like nausea and hunger.
Many times when a parent is perplexed by their child’s eating disorder we discover that the missing piece is high sensitivity. If your child is an HSP, they need a higher level of patience, understanding, and support when eating. Once this understanding is incorporated into treatment, recovery may become easier.
Highly sensitive kids and eating disorders
Kids who are highly sensitive are at high risk of being overstimulated by food and eating. Common symptoms include:
Picky eating
Food aversion
Food refusal
Refusing to eat in public places
Refusing to eat with the rest of the family
Tantrums during meals
Throwing food
Criticizing/complaining about food and other people at the table
Under-eating (appetite and digestion are both affected by overstimulation)
Binge eating (either as an attempt to cope and/or when overstimulation has caused under-eating and the body needs a high volume of calories to compensate)
Weight loss/gain
What is high sensitivity?
A highly sensitive person (HSP) registers and processes more sensory information from their five senses, their internal organs, and other people’s emotional states. As a result, they often have strong reactions to things that individuals with typical nervous systems barely notice.
It’s important to note that HSPs are not being dramatic or making things up. Their highly sensitive nervous system is a biological and genetic feature. It’s found in approximately 20-30% of humans, as well as over 100 other animals, ranging from fruit flies to primates.
Being highly sensitive is a biological trait that carries both positive and negative aspects. On the positive side, many inventors, explorers, artists, musicians, and critical thinkers are HSPs.
Some notable individuals who exemplify HSP traits include Abraham Lincoln, Jane Goodall, Princess Diana, Albert Einstein, Emily Dickinson, and many more. Being highly sensitive is truly a gift that enriches not only the individual but also their family, community, and society as a whole.
However, their highly-sensitive nervous systems put HSPs are at risk of becoming overwhelmed. Eating is particularly stimulating for HSPs, so they often are picky eaters with intense food aversions and can develop disordered eating and/or eating disorders.
We live in a highly stimulating and unnatural environment, so HSPs face a higher risk of experiencing anxiety, depression, eating disorders, and substance use disorders. However, these conditions can often be managed or even eliminated when parents help HSPs learn effective strategies to regulate their emotions.
HSP traits
Here are three key traits associated with being highly sensitive that might lead to an eating disorder:
Extreme noticing: HSPs have a heightened awareness and perception of the sensory information bombarding their nervous system. They notice and react to more subtle details that others may overlook. For example, they may experience intense discomfort from an imperceptible itch in a seam, be highly sensitive to certain sounds, or feel nauseated by specific sensory aspects of food. Eating, which engages all senses, can be particularly overstimulating for HSPs.
Emotional contagion: As social beings, all humans possess mirror neurons that enable them to pick up on the emotions of others. HSPs have a greater number of mirror neurons in their brains, resulting in an increased sensitivity to nonverbal emotional cues. If someone close to them, like a family member, friend, or teacher, is emotionally dysregulated, HSPs often feel the same dysregulation. This heightened emotional contagion can make various social experiences, such as family dinner tables, school cafeterias, and restaurants more challenging for highly sensitive people.
Overstimulation: With their heightened ability to process sensory information, HSPs are more susceptible to being overwhelmed by information from both internal and external sources. This means that things like noise, smells, light, other people’s emotions can quickly become overwhelming for them. Additionally, internal sensations such as upset stomachs, nausea, physical pain, and anxiety symptoms are intensified in HSPs. When overstimulated, highly sensitive individuals may exhibit behaviors that seem like overreactions to others, such as refusing to eat, throwing food, and extremely picky eating.
HSPs and neurodivergence
In our ancestral environment, the heightened sensory abilities of HSPs were essential for detecting threats and protecting the tribe. However, living in our modern, noisy, and overstimulating culture can be overwhelming for highly sensitive individuals.
Due to the unique wiring of their nervous systems, HSPs can fall under the category of “neurodivergent.” Importantly, not all HSPs have formal diagnoses for conditions like autism or ADHD. Nevertheless, it’s common for them to relate to some of the symptoms associated with these conditions.
It’s important to recognize that being highly sensitive is a biological trait. It is not a disorder or illness. However, HSPs benefit from developing skills that help them cope with our overstimulating environment. This is especially true if they’re struggling to eat.
How to help your highly sensitive child with an eating disorder
If you suspect that your child may be highly sensitive, one of the most effective ways you can support them is by helping them develop emotional regulation skills. Many highly sensitive individuals express a need for downtime to rest and recover from stimulating experiences. They also thrive with clear boundaries to protect them from emotional contagion. Finally, they need the freedom to explore their rich inner world on their own terms. Here are important ways you can help:
Teach them emotional regulation. All children are born with immature nervous systems, and parents are essential in teaching kids to regulate their emotions. If you have a highly sensitive child, they need a high level of support and skill-building. You can help them learn how to regulate their nervous systems given their unique biology.
Support them with eating. A highly sensitive child who has an eating disorder needs a lot of support. You can help them learn how to eat in a more regulated way. Remember that they taste and experience food differently from others. Validate their unique experience even as you insist upon eating enough food, often throughout the day. Both parts (validating and boundaries) are essential to eating disorder recovery. This is a skill you can learn and practice every day as you support your child in recovery.
Accept (and nurture!) their quirks. Highly sensitive people perceive the world differently. This is a major strength and is why so many notable figures in history have highly sensitive traits. Don’t try to turn your highly sensitive child into a typical child. Instead, nurture their unique strengths and support them in finding their way in the world with (not in spite of) their beautiful differences.
Ginny Jones is the founder of More-Love.org, and a Parent Coach who helps parents who have kids with eating disorders.
Complex trauma is trauma that happens over a long period of time, often beginning in early childhood, and it’s strongly associated with eating disorders. Traumatic experiences range from physical and verbal abuse to less-obvious but still deeply damaging behavior like criticism, emotional neglect, weight teasing, food insecurity, and food shaming.
Complex trauma can lead to a syndrome called C-PTSD or complex post traumatic stress syndrome. PTSD, which is more commonly discussed, is event-based. It shows up following events such as an accident, assault, or natural disaster. However, C-PTSD is layered into a child’s life, sometimes from birth.
How complex trauma leads to eating disorders
People who identify as having complex trauma are affected as much by what did happen, such as teasing, criticism, and physical violence, as what did not happen, such as unconditional positive regard, emotional caregiving, and support.
All children need emotional caregiving from parents. However, many parents aren’t raised in an emotionally nurturing household and therefore don’t have the skills to provide it to their own children. Thus, complex trauma often happens even when parents have the very best intentions. Almost no parents intend to cause complex trauma, and yet its effects are devastating and can lead to eating disorders and other problems.
Both PTSD and C-PTSD have chronic symptoms, including flashbacks, depersonalization, and dissociation. A person with these symptoms will naturally reach for coping methods, which range from zoning out, avoiding events, people, and situations, and behaviors like eating disorders, substance use, and self-harm.
Researchers say that “the eating disorder may function as a survival mechanism, and may have a protective function to avoid the emotional confrontation with the trauma experience.” Here are a few true stories of complex trauma and eating disorders:
Jenn’s story
Jenn’s eating disorder started, as so many do, with a diet. Her mom took her to Weight Watchers starting at age 9. Today, at age 38, she is married and has a 3-year-old son, and she started serious treatment for her eating disorder last November. “I see an eating disorder therapist and a dietitian, which is required by my therapist, twice per week,” she says. “This takes the food out of therapy so we can focus on the trauma.”
Jenn believes that complex trauma was the catalyst for her 30-year eating disorder, which began at age 9, alongside those Weight Watchers meetings. She’s now in recovery and is working on her PTSD. She didn’t believe she had PTSD at first. “My therapist said ‘you have complex PTSD,’” says Jenn. “And I said ‘that’s not a thing, I wasn’t in a war!”
Yet after further work with her therapist and reading about C-PTSD all the symptoms lined up. “Getting help consistently has been the best thing I’ve done,” says Jenn. “I’m someone who’s experienced significant trauma and experiences intrusive thoughts all the time – all day, every day. I thought this was all part of my personality. Growing up I thought this is just who I am. Now I realize there’s so much more going on.”
Like so many adults with long-term eating disorders, Jenn is dealing with paying for treatment herself. “My therapist is extraordinary,” says Jenn. “I’m paying for both her and my dietitian out of pocket, which isn’t great, but it needs to happen. I have a son and it’s really important for him to not have to worry about the things I’ve dealt with.”
Tina’s story
Tina remembers first restricting food at around 9 or 10 years old. “When I did eat I had very few safe foods and I’d almost always eat alone,” she says. Today, at age 37, she says she’s healing from both her eating disorder and complex trauma. “I am 37 and I finally, for the first time in my life feel free of my eating disorder,” she says. “I don’t like ‘healed;’ that feels false. My anorexia and body image issues will likely always be with me in some way but I don’t believe my anorexia-driven thoughts and feelings anymore.”
Tina sees her eating disorder as intrinsically linked to the complex trauma she experienced. “Given the situation at home, I was going to develop a coping mechanism,” says Tina. “My eating disorder is how that manifested for me. My sister is a perfectionist who attempted suicide in high school. And my brother struggled with alcoholism and self-harm and died by suicide last year. My eating disorder may very well have saved my life.”
While this idea may surprise you, many people with complex trauma and an eating disorder see their disorder as the only way they could cope with their life. Tina describes her eating disorder as a way to “not know” about how bad things were for her and her siblings at home. “The not knowing made it tolerable,” she says. “If I knew how love should feel I would have known I was starving in more than one way.”
Tina began healing from complex trauma and her eating disorder by reaching out to her sister. “We were able to hear and validate our experiences as children and as adults with our parents,” she says. “This was invaluable. We sought out literature together and slowly learned about emotional neglect, abuse, and complex trauma. We are both in therapy now.”
“Healing has felt emotionally what I assume waterboarding must feel like physically,” she says. “At every turn I feel like l will surely die, that the pain is too great and then, I do not die. I learn I have more capacity than I knew and I can trust my body.”
Tina has found validation, meditation, breathwork, and finding ways to feel safe in her body most helpful. “Emotional flashbacks are so difficult,” she says. “Meditation and being present in the moment, in my body, is my lifeline.”
How parents can help kids with complex trauma and eating disorders
If your child has both complex trauma and an eating disorder, you can make a big difference. Your child’s mental health and eating disorder recovery will depend on their ability to process their complex trauma. Keep the following ideas in mind as you help your child heal:
Do not debate the validity of your child’s memories of their childhood. That will only hurt them more.
Listen and be compassionate to their experience of their childhood.
Your job is not to correct your child’s memories, but to compassionately witness their memories and hold them in ways you were unable to before.
If your child asks you to go to therapy with them, go.
Get yourself a therapist or coach who can work through your own trauma of supporting a child who has complex trauma. You deserve a safe space to work out your feelings about this. You will be better able to support them if you get support for yourself.
Keep in mind that most children who have complex trauma have parents who have complex trauma. It tends to run in families. Have a lot of compassion for yourself in this process. It didn’t start with you, and together you and your child can end the cycle of complex trauma.
This is hard for everyone, but never doubt the transformative potential of sitting with your child in their pain and grief. Your ability to do so is beyond powerful. And while you may not want to face this, doing this can result in a deeper, more meaningful relationship with your child.
Ginny Jones is the founder of More-Love.org, and a Parent Coach who helps parents who have kids with eating disorders.
Jill is beside herself with worry. Her daughter Melody has an eating disorder and is struggling with loneliness. Between treatment, COVID restrictions, and starting high school, she has become very isolated. “She has always been more on the introverted side,” says Jill. “But it’s gotten to the point where I’m pretty sure she doesn’t have a single good friend.”
“She has people she talks to in class,” says Jill. “But there’s nobody she can call or share notes with or hang out with after class or on the weekend. I think that loneliness is making it harder to recover from her eating disorder. But loneliness is also partly driven by the eating disorder. I don’t know what to do.”
Jill’s worry makes a lot of sense. And she’s right that loneliness is both a contributing factor to and a symptom of an eating disorder. Melody is naturally introverted. But she’s also been hit with a triple whammy: a pandemic, the transition to high school, and eating disorder recovery.
Loneliness and social isolation
Loneliness is a major factor in mental and physical health. In fact, social relationships are the most important lifestyle factor in longevity. Social connections are even more important to health than avoiding tobacco and alcohol. Humans are social beings, and connecting with others is essential to our health and well-being.
How to help a child who has an eating disorder decrease loneliness
Of course parents like Jill desperately want their kids to form social connections and feel a sense of belonging. This is especially important during the teenage years, so it’s understandable that Jill is concerned. But what can she do? How can Jill help Melody reduce her loneliness during eating disorder recovery?
The first thing to know is that every person has a different need in terms of social connections. And while most of us think about a large pack of kids getting together on the weekends, it’s perfectly acceptable if your teenager has just one or two good friends. In fact, set your sights very low: one.
“The biggest return we get in friendship is going from zero to one friend in terms of its impact on our mental health and well-being,” says Marisa Franco, author of Platonic: How the Science of Attachment Can Help You Make — and Keep — Friends. “If you can get that deep with one person, it’s going to be powerful and it’s going to be impactful, and you don’t need to have a ton of friends.”
Taking the pressure off having a large number of friends can be a great place to start. Find ways to weave this idea into your conversations with your child. You can talk about your own friends individually vs. as a group. And when your child complains about having no friends (plural), help them understand that just one friend would be awesome. Encourage them to look around for just one person at school who they can eat lunch with. Set your sights low, and normalize the idea of just one friend.
2. Family relationships
Your child wants and needs peer friendships, but that doesn’t mean they can’t get a lot of benefits from their social connections with family.
Our first social group is our family. How strong are your family ties? Does your child feel integrated and as if they “belong” to your family? Start by building family traditions and telling stories that help your child see how they fit into the family. Spend time building family integration every single day. A great place to begin is a family meal, which has countless health benefits, probably in part because of the social belonging it builds.
If possible, schedule activities with extended family members. It’s OK if you don’t have a strong connection with biological family – can you build a family of friends? Do what you can to expand your child’s social interactions within the scope of your family. And don’t forget to help them integrate into family activities. This may be uncomfortable if your child is feeling lonely and vulnerable, but parents can help grease the wheels of interaction!
3. Social skills
If your child is struggling with loneliness and an eating disorder, combined with COVID and a major transition like starting high school, they may need to brush up on their social skills. This can be a tricky area for parents to get involved, but the first thing to consider is whether your family is upholding and modeling good social skills.
Many families slip into dysfunctional patterns of not being friendly, not speaking politely to each other, not managing their emotions, and acting out against other family members. If you see these dynamics in your family, then get some coaching or family counseling to work on interpersonal boundaries and emotional regulation. Before you decide that your child is the one who has a problem with social skills, consider whether this is a family dynamic. It will hurt your child’s chances of success if you treat a family problem as if it is a personal failure.
Next, talk to your child about social skills. The easiest way to do this is to talk about your own experiences or use characters on TV and movies. Ask questions like: How would that behavior make you feel? What do you like about that character? How do you think that character could be a better friend? Remind your child that relationships can’t be adequately portrayed in the media, and that just like bodies, we need to take media relationships with a grain of salt.
4. Formal social groups
Teens have undergone tremendous upheaval in the past few years, and lots of them are struggling with loneliness. This is the perfect time to use formal social groups and organizations to help support social development. Ask your child to investigate clubs at school.
Many schools have a wide variety of clubs that appeal to a broad array of personalities and interests, but you can also look for clubs in the community and at your place of worship if you have one.
Encourage your child to join at least one club. This may require some well-placed parental pressure. Someone who is lonely may resist the idea of joining a club because they are stuck in a cycle of feeling low. It’s OK for you to insist on some participation. You can’t force your child to go, but don’t underestimate the power you have to influence them to give it a try. Sometimes lonely kids need a lot of verbal encouragement and requests to get out of their rut.
5. Get help
If you do all these things and your child’s loneliness is not lifting at all, then you and your child need more help. Talk to your child’s eating disorder care team. They are probably as concerned about loneliness as you are. Find out if they have any suggestions or can help your child get involved in activities. Sometimes having a non-parent make these suggestions is the key to getting them done.
A worthy focus
Loneliness is a contributor to the psychology of an eating disorder, so supporting them in addressing this is a worthwhile activity. You want to understand your child’s loneliness and support them in feeling better. Loneliness has been correlated with eating disorders and other mental disorders. It is also correlated with the No. 2 and No. 3 mortality factors: tobacco and alcohol addiction.
Jill was relieved to know that she wasn’t being silly worrying about loneliness. “There was a part of me that thought maybe I was worrying about nothing,” she says. “Or that this is none of my business. But now I feel as if my worries make sense, and I’m going to take some action to start helping Melody feel better.”
Ginny Jones is the founder of More-Love.org, and a Parent Coach who helps parents who have kids with eating disorders.
Monique is very worried about her daughter Maya. After a few years of struggling to deal with stress, Maya is now deep into an eating disorder. Monique and her husband Leonard are dedicated to helping her recover, but they are worried that stress is a major ongoing problem.
“I worry that unless we address her stress, she’s still going to struggle,” says Monique. “Eating disorder treatment is hard, and it seems to me like if we don’t figure out how to reduce her stress, we’re just treading water with her mental health. I just don’t know what to do about it.”
Maya, 16, has always been a sensitive child. “When she was a toddler, she was really picky about her food and clothing,” says Monique. “So I adjusted her diet and made sure I didn’t buy her any clothes with tags. She seemed to do OK for years, but when puberty hit, she started spiraling into stress. Now it seems like she just can’t handle life, and it’s not as simple as it was when she was little and I could control everything and reduce the stressors.”
Everything that Monique says makes sense. And she’s right: without addressing Maya’s struggles with stress, it will be hard to achieve eating disorder recovery and, ultimately, mental health.
Why so stressed?
To get started, I asked Monique some questions about what stresses Maya out. Based on her childhood experiences, it sounds like Maya is a highly sensitive individual. This means that she is naturally more sensitive to stressors. But what exactly is creating so much stress for Maya right now?
I started by defining the three types of stress and how they appear when a person has an eating disorder. Stress is an important part of the psychology of an eating disorder. The three types of stress are:
1. Healthy stress
Not all stress is bad! We need stress to learn and grow. Without stress, we would never achieve maturity. This stress is healthy and adaptive, but that doesn’t mean it’s comfortable. In fact, healthy stress can trigger all the troubling signs of emotional dysregulation, including yelling, crying, and avoiding tasks that seem impossible. However, when a person faces their healthy stress with courage, their struggles build emotional resilience and maturity. A person cannot mature without healthy stress!
It’s not really the type or size of the stress that you experience but your ability to cope with the stress that defines whether stress is helpful or toxic.
Some forms of healthy stress that your child must navigate if they have an eating disorder include:
Eating enough food
Eating regularly throughout the day
Body changes (e.g. weight gain)
Going to therapy, medical, and nutrition appointments
Disagreeing with parents and siblings
Being assertive about needs and boundaries
Going to school
Completing difficult school tests and assignments
Studying
Having reasonable expectations of extra curricular activities
Making new friends and socializing
Having social media limits
Getting to bed at a healthy time each night
🔑 The key if your child is experiencing healthy stress is to validate their experience (e.g. “this is hard”) while also expressing confidence in their ability to handle it (e.g. “I know you can handle this.”). Seek ways to support your child through healthy stress daily, and get coaching and support if this is a struggle for you.
2. Traumatic stress
This sort of stress is related to a specific event or action. It overwhelms a person’s coping resources and may become stuck if not processed. Common forms of traumatic stress include:
Serious accident
Physical or sexual assault
Physical or emotional abuse
Exposure to traumatic events at home, including domestic violence
Serious health problems, such as heart surgery, cancer, etc.
Having a sibling or parent with a chronic illness (physical or mental)
The death of someone close, such as a parent or sibling
Divorce
Vomiting, choking, and painful gastrointestinal episodes
The interesting thing about traumatic stress is that it doesn’t impact everyone equally. Two people can face the same traumatic event, and one may develop traumatic stress symptoms while the other may not. The difference between ongoing symptoms after traumatic stress is whether the event is processed healthily. Some people can do this by themselves, but many others need a lot of emotional support to process a traumatic event.
For example, many kids get through their parents’ divorce without any PTSD, while others need some help processing their feelings about the divorce and its impact on the family.
🔑 If your child is experiencing traumatic stress, the key is to get them professional support to process their trauma. A therapist specializing in PTSD will support your child in facing their fear and overcoming the long-term impacts of traumatic stress. You can also learn skills to respond to your child’s PTSD appropriately.
3. Chronic stress
Chronic stress builds over time. A person experiencing chronic stress often feels stuck and unable to make changes to improve their life. This sort of stress is often entrenched and hard to break out of, but parents can help. According to Yale Medicine, some symptoms of chronic stress include:
Aches and pains
Insomnia or sleepiness
A change in social behavior, such as staying in often
Low energy
Unfocused or cloudy thinking
Change in appetite
Increased alcohol or drug use
Change in emotional responses to others
Emotional withdrawal
Common stressors to be aware of in your child’s life include:
Difficult family relationships, especially with parents and siblings
Lack of sleep
Lack of family structure and support
A heavy workload at school
Pressure to achieve certain grades and achievements
Intense sports activities/expectations
Pressure to perform at very high levels at school or in extracurricular activities
Bullying
Overuse of social media
Chronic stress needs to be addressed to recover from an eating disorder. Your child’s lifestyle must change to reduce chronic stress and build experiences of healthy stress.
🔑 There are two keys if your child is experiencing chronic stress. The first is to reduce unnecessary stressors in your child’s life. This can begin by looking at their schedule and removing non-essential activities and pressure to perform. The second is to turn the necessary stressors of life (e.g. eating, going to school) into healthy stress. With the right approach, you can help your child gradually turn chronic stress about eating and other stressors into healthy stress.
Maya’s stress and eating disorder
I reviewed Maya’s stress with Monique using a worksheet I created. Together, we identified three primary issues that need to be addressed right away:
Eating Stress (chronic)
Maya feels tremendous stress about eating. She is worried about food all day, and it is hard for Monique to calm Maya enough to get the nutrition she needs to recover.
🔑 This is chronic stress that can be turned into healthy stress. In combination with Maya’s eating disorder treatment team, Monique can support Maya and help her face the stress of eating with courage and determination. Over time, she will learn to face eating and mealtimes as healthy stress. While eating may continue to be challenging for her, she can transform it from chronic stress to healthy stress.
Sibling Stress (chronic/traumatic)
Maya and her brother Victor have a negative relationship. Victor is aggressive with Maya and frequently criticizes her. Sometimes he even gets physically violent and pushes or pinches her.
🔑 This is chronic stress that needs to be eliminated. Monique and Leonard need to immediately seek therapy for Victor and set firm boundaries around how he treats his sister. Monique and Leonard must intervene whenever they observe Victor being aggressive, critical, and violent with Maya. There should be a zero-tolerance policy for these behaviors in the household. Additionally, they should have Maya see a trauma specialist who can determine how best to address any trauma resulting from her brother’s treatment.
Performance Stress (chronic)
Maya feels overloaded with homework and tests. She has a lifelong dream of attending an Ivy League university. The pressure to perform has become overwhelming, and Maya spends hours trying to motivate herself to do homework and study. Her grades have been steadily slipping, and she often stays up until 2 a.m. trying to complete her work.
🔑 This chronic stress needs to be adjusted. While academic goals can be a healthy form of stress, it is clear that they have crossed the boundary and become chronic stress. Maya needs support from her therapist to re-evaluate her goals and get healthy study habits and boundaries in place. Monique and Leonard should meet with Maya’s school counselor to determine reasonable expectations and help Maya manage her academic goals.
Moving forward
Understanding Maya’s stress helps Monique and Leonard see how stress affects Maya and how they can help her start having less toxic stress in her life. Knowing the three types of stress affecting eating disorder recovery has given them the confidence to start making changes at home and in Maya’s treatment program.
Ginny Jones is the founder of More-Love.org, and a Parent Coach who helps parents who have kids with eating disorders.
For privacy, names and identifying details have been changed in this article.
If your child has an eating disorder, recovery means more than simply gaining weight and/or stopping eating disorder behaviors; it means becoming mentally healthy. Eating disorders are frequently misunderstood, and people don’t always realize that mental health, not just eating disorder recovery, is the goal.
That’s why I’ve put together a mental health checklist to help you set expectations and goals as your child recovers from their eating disorder. This mental health checklist is especially important if your child is returning to college or independent living after undergoing recovery in your home and/or a treatment facility.
Eating disorders are often layered on top of poor mental health and other mental disorders, so if parents don’t pay attention to mental health overall, they risk having a boomerang effect of having a child leave and return to eating disorder treatment. While you can’t control their recovery, you can do your best to set your child up for success. Nobody wants your child to feel they are ready to return to independent living or go to college only to discover that they are not yet equipped to care for themselves, so the more you can help them build the skills they need to be mentally healthy, the better. A mental health checklist to be used during and after eating disorder recovery can help.
Mental health sometimes feels arbitrary. But in fact, we can measure mental health based on the behaviors that lead to and indicate mental health. It’s just like eating disorders. Except for medically-underweight anorexia, eating disorders don’t often have measurable physical symptoms. Instead, they are diagnosed based on the behaviors observed.
For example, eating disorders are measured by how often a person eats, how much they eat, and how they feel about eating. Similarly, mental health can be measured by how well a person takes care of themselves and how they feel about themselves.
In addition to your child’s recovery process, they should be learning to take care of their physical health, which includes at a minimum:
Getting adequate food and water
Moving their body appropriately
Getting enough sleep
Basic hygiene
Beyond basic physical healthcare, your child should also take care of their emotional health, which includes at a minimum:
Connecting with others
Managing social media use
Practicing mindfulness
Getting outdoors
Asking for help
Taking breaks
Having self-compassion
Physical self-care after an eating disorder
Even if your child is cleared of an active eating disorder diagnosis, they are still at risk of mental illness. They will need to care for their bodies and minds intentionally for life. This is important for every person, but particularly for someone who has/had an eating disorder. Here are the basic physical care steps that your child should take to improve mental health.
Getting adequate food and water
All bodies need enough food and water to function. And a lack of food and water has a significant impact on both mental and physical health. When someone has/had an eating disorder, it’s an indication that they may need to be more vigilant than others about caring for this most basic element of self-care. As your child transitions to living independently from you, they should demonstrate an ability to feed themselves adequate quantities of food every 3-4 hours and drink at least 6-8 glasses of water daily.
Moving their body appropriately
Our bodies are made to move. Regular movement is essential to both physical and mental health. The tricky part is that many people who have eating disorders incorporate excessive exercise and/or are at risk of serious health complications if they exercise. However, as your child recovers from their eating disorder, they should work in regular movement to maintain health. This can be functional like having a walking commute to work or school, going for a short walk each day, doing a brief home exercise routine, or joining a gym or attending fitness classes. Your child should demonstrate an ability to move their body regularly, not too much and not too little.
Getting enough sleep
Getting enough sleep is a cornerstone of mental health. Your child needs 8-9 hours of sleep per night. People with eating disorders and other behavioral and mental health problems often experience sleep loss. Your child may have insomnia or struggle to settle down and get to sleep. While it’s easy to dismiss sleep as unimportant, it is as important as food, water, and movement to the human body and mental health. Sleep loss is no joke for anyone, but it is particularly risky for someone who has been diagnosed with a mental disorder like an eating disorder. Losing sleep is a major risk for someone with a history of mental disorders. Therefore, your child should demonstrate an ability to get adequate sleep each night and wake up at an appropriate hour in the morning.
Basic hygiene
While basic hygiene may seem like a given, it can be a major struggle for someone with an eating disorder, anxiety, depression, or other mental disorder. On the one hand, if your child has OCD, they may lead towards overdoing hygiene. Some people will wash and clean themselves excessively. On the other hand, someone who is depressed or has ADHD may feel unable to clean themselves adequately. Either way, taking care of basic hygiene is essential to mental health. Like exercise, you’ll need to measure whether your child’s challenge is doing too much or too little and work from there. Set some basic expectations, like flossing and brushing teeth twice daily. Bathing can vary per person, but discuss the maximum number of days between showers and/or the maximum number of showers per day. Your child should demonstrate an ability to take care of their basic hygiene.
An eating disorder is a mental illness. This means that while physical symptoms and/or behaviors are used to diagnose an eating disorder, it is emotional and mental in nature. This means that your child needs to care for their emotional health. This is important for everyone, but particularly for someone who has/had an eating disorder. Here are the basic emotional self-care steps that your child should take to maintain their mental health.
Connecting with others
Human connection is as important as food, water, sleep, and movement. It is a sign of mental health to reach out to other people. It doesn’t have to be lengthy or intense. Still, you should feel confident that your child has some human connection daily. It might be a phone call to a loved one, but it could also be as simple as going in person to get groceries or food and speaking to someone while getting it instead of ordering contactless delivery.
Managing social media use
Social media can be a major impediment to mental health for numerous reasons. It is particularly dangerous for people who have/had eating disorders due to the algorithmic preference for very thin people who promote “healthy lifestyles” that include eating disorder behaviors and beliefs. While zero social media use might be ideal for mental health, it’s not realistic or necessary for most people. Your child should demonstrate that they can set limits on their usage.
Practicing mindfulness
One of the symptoms of an eating disorder is a disconnection between the mind and the body. It’s as if the brain-body connection is severed. To recover and maintain mental health, your child needs to practice a mindful connection between the brain and body. Your child should have a daily mindfulness practice that actively connects the brain and body.
Getting outdoors
Studies have shown that being in nature, even for a few minutes daily, has numerous physical benefits, including less pain and lower diastolic blood pressure. It improves mood and reduces the risk of mental illness. Support your child in getting outdoors for at least a few minutes daily. They can combine this with either exercise or mindfulness, or both. They should take a few moments to feel the air in their lungs and look at the sky, a tree, or anything natural and not human-made.
Asking for help
There is a tendency when someone has a mental disorder like an eating disorder, anxiety, depression, etc., to self-isolate. They reach out less to people who care about them and say less about how they are feeling. You want to support your child in reaching out for help when they feel sad, scared, or angry. Nobody can take their feelings away, but sharing our feelings with other people is soothing and improves mental health.
The brain-body disconnection common in eating disorders often translates to ignoring signs of mental or physical fatigue. A mentally healthy person recognizes when they need a break and takes breaks to improve their health and performance. Help your child learn to take breaks when they are overwhelmed or having physical or mental symptoms of fatigue.
Having self-compassion
A mentally healthy person has compassion for themselves. They don’t beat themselves up when they make mistakes and don’t speak cruelly or dismissively to themselves. They know how to soothe themselves when things go wrong and treat themselves as they would a good friend. Help your child learn to speak to themself with self-compassion and love.
Giving your child a mental health checklist for eating disorder recovery
Discussing mental health with your child while they are still recovering from an eating disorder and preparing to leave your daily care will help them build mental health. You can create your own checklist or use the one I created. The checklist I created includes both daily actions and warning signs to keep in mind. You can provide this to your child and talk with them regularly about both elements: are they doing daily self-care, and are there any warning signs to address? This can help you communicate your concern for their mental health, even if your child isn’t living with you.
Ginny Jones is the founder of More-Love.org, and a Parent Coach who helps parents who have kids with eating disorders.
If your child in in recovery for an eating disorder, it’s very possible that they feel sad. And maybe this is making you sad, too. Most parents feel overwhelmed handling the eating disorder behavior, and don’t know what to do when sadness shows up.
As parents, we want to protect our children from uncomfortable feelings, especially sadness and despair. Most of us came into parenting during the time of a glut of Happiness books, speeches, and articles. Scientists explored exactly how we can increase our happiness with daily tasks, based on the assumption that being happier is always better.
Most of us, when asked, will say that what we want most of all is for our kids to be happy.
We may embrace sayings like “good vibes only” and strive every day to turn lemons into lemonade. When our children feel sad, we jump through hoops to try and remedy it as soon as possible – to return to happy.
The tyranny of happy
It sounds really nice to pursue happiness, but the fact is that many of us who pursue a happier life find ourselves actually feeling emptier and sadder. Why?
Because it turns out that sadness is a part of natural emotional hygiene. To expect ourselves – and our children – to live in a state of perpetual happiness is to deny the natural fluctuation of emotions.
Feeling sadness and any negative emotion is not only normal, it’s actually healthier than trying to force ourselves to remain in a constant state of bliss.
When we have a child who has an eating disorder, it’s hard not to think that we need to help our child find a higher state of happiness in life. We may think that recovery from their eating disorder will mean a return to happiness.
Certainly, if our child is depressed, we should seek treatment for that condition. But the opposite of depression is not eternal happiness. The opposite of depression is the ability to feel a full range of emotions, including sadness.
Recovery from an eating disorder does not mean happiness all the time or never feeling sad. It means we recognize and metabolize the full range of emotions including, but not limited to happiness. This means we need to feel free to experience anger, sadness, loneliness, jealousy, and the thousands of other emotions that make us human.
Parents who are afraid of the full range of human emotions are likely to get uncomfortable with this. They may accidentally try to interfere with natural emotional ranges by pursuing happiness rather than allowing sadness and other negative emotions.
But parents need to accept all mood states, not just the positive ones.
Acknowledge feelings
The first step in learning emotional hygiene – the natural metabolism of emotions throughout each and every day – is to acknowledge that our emotions run a wide range. We have to acknowledge that we are not meant to remain in a steady emotional state.
In fact, that is a clear sign of depression: the lack of emotional fluctuation. Take some time in your family to acknowledge that feelings come and go every single day. We all have a broad range of positive, negative and neutral feelings, and that is absolutely healthy.
Name feelings
Building emotional literacy, or the ability to put a name on your emotions, helps to build emotional resilience and reduce shame around negative emotional states. When we talk about our feelings, we allow them to exist without worrying that they will last forever. Talking about emotions is a daily practice that we can all work on in our families.
Some of us find it helpful to print out lists of emotions to help us name them. It’s too easy to call every negative feeling afraid, angry or sad. And that’s certainly a good place to start, but there are so many nuances to those feelings. We can add words like despair, fear, horror, and shame to help us better define our feelings. This will allow them out into the light where they can breathe and move on.
Don’t forget that sometimes we need to combine feelings to get an accurate picture. For example, before a big event, a child may say they feel scared. But upon deeper reflection, they are a combination of nervous and excited. You can even put these words together to form new feelings, like “nercited.”
Welcome feelings
Even if we are able to name our feelings and have a broad emotional vocabulary, we still have to work hard to welcome the negative feelings into our lives.
Almost all of us were taught to reject, deny and ignore negative emotions. A good reason for this is that negative feelings make parents very uncomfortable.
As little children, our parents, in wanting what was best for us, probably tried to get us to stop crying. A better approach would have been to welcome our tears and reassure us that they were perfectly natural and healthy. These lessons learned every day for many years, taught us to hide negative mood states.
We can learn to welcome the full gamut of our family’s feelings. Every member of our family is going to undergo mood states throughout the day. And a good portion of those feelings are going to be in the negative category.
Rather than not allowing negative feelings or trying to pretend that everything is just fine, practice instead welcoming these feelings.
Talk about the fact that life is challenging.
Sometimes it sucks.
But it will suck much, much more if feelings are repressed. In fact, repressed feelings are integral to almost all addictive and maladaptive behaviors, including eating disorders. Sadness is a common psychological symptom of eating disorders. Emotions run high in eating disorder recovery, so most people will be sad at times. But this doesn’t mean recovery is a failure. It means that recovery opens up a person to the full range of human emotion. And this is a sign of mental health.
Ginny Jones is the founder of More-Love.org, and a Parent Coach who helps parents who have kids with eating disorders.
Body autonomy, the simple but powerful right to have control over one’s own body, is something every child deserves. Yet when a child struggles with an eating disorder, that sense of control can feel shattered or tangled in complex ways.
Understanding the connection between body autonomy and eating disorders is key for parents who want to support their child’s recovery in a respectful and empowering way. This parent guide will explore how struggles with control and autonomy show up in eating disorders, why honoring your child’s sense of self matters, and practical ways you can help nurture their independence while guiding them toward healing.
Body autonomy and eating disorders
Terri is worried. Her 14-year-old daughter Natalia had been struggling with an eating disorder for over a year. Terri feels like a helpless bystander and the whole family is suffering.
“Natalia was always so diligent, kind, and helpful,” says Terri. “I never thought she would be the one to struggle with anything. It seemed to me like she was doing so well. But now everything has been turned upside down.”
In addition to the terrifying eating disorder behaviors, Terri has also noticed that Natalia is dressing very differently and has developed a passion for tattoos and body piercing. “It’s all she can talk about,” says Terri. “She spends so much time looking at tattoos and piercings on TikTok. It’s become this new wild passion. She’s wearing dark, torn clothing and wants a green mohawk! She just looks nothing like the girl we knew before.”
I can understand Terri’s concerns, and I also sense that perhaps something related to identity and bodily autonomy is going on. In fact, eating disorders can be seen as a pursuit of bodily autonomy, so this is not unusual. But we need to understand why Natalia is seeking to assert her bodily autonomy. This will help us know how to help her feel better.
Eating disorders and bodily autonomy
It’s not uncommon for eating disorders to overlap with a pursuit of bodily autonomy. Seeking to change your body and control what it does and how it looks makes perfect sense, especially during adolescence. It’s a natural part of human development to test boundaries and try on different identities. But when trying things out involves a drastic change in appearance, using eating disorder behaviors, or otherwise interferes with life, we obviously want to understand more.
It’s not uncommon for people who have an eating disorder to also alter their bodies in other ways. More conventional people may spend time styling their hair, perfecting their makeup and nails, and finding the ideal outfit to fit in with their peers. On the other hand, less conventional teens may become interested in alternative clothing, hairstyles, piercings, and more. Of course, these teens are also “fitting in” with an image, just in a different way from the more conventional teen.
What we want to consider is whether their attention to appearance is normal teenage behavior. Or is it a deeper attempt to assert bodily autonomy?
Bodily autonomy is having ownership over your own body.
Bodily autonomy is an important part of developing into an independent and mentally-healthy person. It can be impacted by situations in which a person doesn’t feel they are in control of their own body. As a result, some people don’t feel they “own” or are in charge of their own bodies. They may seek to claim ownership through appearance and eating disorders.
Some reasons for low bodily autonomy include:
Sexual trauma
Physical abuse
Medical trauma (even though they are life-saving interventions)
Bullying
Accidents such as nearly drowning, car accidents, bike accidents, etc.
Beyond these personal incidents, bodily autonomy can also be impacted by broader social conditions such as:
Laws that prevent people from making decisions about their own body (e.g. anti-abortion laws, anti-gay-marriage laws, anti-trans laws, etc.)
Institutions like patriarchy and white supremacy that devalue groups of people based on their race, gender, sexual orientation, etc.
Beliefs like homophobia and transphobia that demonize people for who they love or which gender fits.
If your child is non-white, female, and/or LGBTQ+, these social conditions reduce their bodily autonomy.
How parents impact a child’s bodily autonomy
Parents may accidentally make children feel they are not in charge of their own bodies. Often this makes perfect sense. For example, when kids are young, parents need to take steps to ensure their child’s safety. But in a highly sensitive child and/or in special cases, these interventions can create a sense of disconnection for the child. These kids need a little extra help to claim ownership of their bodies in a healthy, adaptive way.
There are three main ways that parents can accidentally impact bodily autonomy:
1. Life-saving interventions
Sometimes threats to bodily autonomy are medically necessary. For example, some parents must approve medical surgeries and interventions for their children. It may be a feeding tube for an eating disorder or surgery for a congenital defect. Regardless of why they are necessary, these medical interventions take away the child’s power to control their own bodies.
They are literally life-saving. And they still amount to a loss of bodily autonomy and thus can create trauma for the child. Trauma studies show that traumatic events impact different people in different ways. This is based on a combination of biology and how the trauma is dealt with or processed.
There are some people who are biologically more sensitive to bodily threats and trauma. But even for people who are not extra-sensitive, trauma tends to settle in if it’s not processed. Processing trauma with a professional can go a long way to preventing long-term post-traumatic traumatic stress.
2. Safety
There is a tricky boundary between keeping kids physically safe and allowing them to explore the world. This is an ongoing debate between parenting experts. Think of the difference between the bestselling books Free-Range Kids and Battle Hymn of the Tiger Mother. These promote completely opposite approaches to raising kids.
Free-Range Kids by Lenore Skenazy promotes complete bodily autonomy by allowing children to explore the world freely. Battle Hymn of the Tiger Mother by Amy Chua promotes very low bodily autonomy and high parent monitoring. It even includes rules like no sleepovers.
As with most divisive parenting approaches, something in between is probably a good approach for most kids. They need certain boundaries but should have enough bodily autonomy to feel as if they are in charge of themselves. This is especially important as they grow older. Figuring out these boundaries is an imperfect pursuit – we all do our best.
3. Lack of Awareness
There is a third, surprising way that parents can accidentally impact kids’ bodily autonomy, and it’s lack of awareness and understanding of the conditions that can reduce autonomy. For example, if parents are not informed and talking about racism, sexism, misogyny, homophobia and transphobia, then their child will grow up without the benefit of knowing that these issues are not their fault or a personal failure. They are a failure of our society. On the other hand, if parents talk about and educate their children about racism, sexism, misogyny, homophobia and transphobia, their children are more likely to develop bodily autonomy despite the social conditions. Similarly, traumatic experiences can be overcome if parents are educated about the impact of trauma on the sense of bodily autonomy and actively counteract it.
When eating disorders serve a purpose
There are many ways to look at an eating disorder. And no single view is going to address the full complexity of eating disorders. But one way to see an eating disorder is a way for a child to assert bodily autonomy and independence. As in: “You can’t tell me what to eat! Stop watching me! I’ll do it myself! I know best!”
When I talked about this with Terri, she felt an intuitive sense that we were onto something. “Natalia had a congenital heart defect that we had to have corrected when she was just two years old,” says Terri. “I can definitely see that the stress of having my baby get an operation influenced how I parented her. It caused me to be very anxious about her safety. I think most of it was unconscious. But as I look back, I know that I gave her brother a lot more freedom than I gave her.”
Terri was responding in a natural and intuitive way to the threat of medical complications. It makes perfect sense that, without realizing it, she was more nervous and cautious about Natalia.
When looking through this lens, we could consider how Natalia’s eating disorder behaviors and attention to her appearance were signaling that Natalia was craving her own independent identity. Also, we know that trauma often underlies eating disorders. We could hypothesize that the necessary surgery was likely a traumatic event for her. Trauma can be an issue even if she doesn’t consciously remember the details.
Eating disorder treatment often denies bodily autonomy
Terri also considered the impact of Natalia’s eating disorder treatment so far. “We took her to the emergency room against her will. And that began a series of medical and therapeutic interventions that were necessary but probably traumatic for her,” says Terri. “I’m so confused because we did what we had to do to keep her alive. But now it seems like maybe that made things worse?”
I assured Terri that many parents face this challenge. And she hadn’t done anything wrong. We have a responsibility to intervene to keep our kids as safe as possible. At the same time, while the interventions were medically necessary, they likely created additional trauma for Natalia. Both of these things can be true at the same time.
The solution is not to regret choices already made – they were necessary! Instead, focus on future action to address the trauma. Now that she’s out of medical danger, Terri can get help for Nadia’s trauma and help build her sense of bodily autonomy.
What parents can do to help
Parents can help their kids recover from an eating disorder by understanding the role of bodily autonomy in emotional health. Our ability to feel independent, strong, and in control of our circumstances is important. Parents who empower their children to claim their bodily autonomy will see positive results.
First, ask these questions:
Is my child showing signs of a need for greater bodily autonomy? (e.g. eating disorder, unusual hair and clothes, body modification such as tattoos and piercings, etc.)
Did my child experience trauma? Was there any situation in which they were physically out of control of their own body?
Have I been anxious as a parent and even over-parented in some ways?
Have I given my child ways to assert control over their own life and body?
If any of the above is true, then it makes sense to consider the role bodily autonomy is playing in your child’s recovery.
With these questions, Terri could connect some dots. She saw how situations that were out of her control had resulted in a lack of bodily autonomy for Natalia. This was a major breakthrough for her. We often feel helpless to help our kids until we understand what might have contributed to their troubles. Once we identify why things could be happening, we are better able to help.
Improving bodily autonomy when there’s an eating disorder
Here are some things that parents can do to increase their child’s sense of bodily autonomy:
Work on your own fears and worries. Get some help in building your anxiety tolerance so you avoid passing it along to your child.
If trauma is a factor in your child’s history, seek treatment for the trauma. Talk therapy may not be as effective as somatic (body) therapies for trauma, since trauma is held in the body.
Become educated about and talk to your child about racism, sexism, misogyny, homophobia, transphobia and other harmful and exclusionary systems so they are empowered to claim their right to exist as they are.
Seek ways to increase your child’s bodily autonomy. What choices can you allow them to make for themselves? In what ways can they be responsible for their own life choices?
Look for ways to gain consent and agreement before imposing rules, systems, and structures on your child.
Encourage your child to express themselves through their body without a sense of shame or rebellion. The more we allow healthy self-expression, the less likely it is to become a problem.
Let go of bothersome but not permanent and/or dangerous forms of expression. For example, allow strange clothing, nail polish, and hairstyles – they are temporary and harmless. On the other hand, it’s OK to hold boundaries on things like tattoos and piercings while your child is under 18 if that’s something you feel strongly about.
Consider how your child’s eating disorder treatment may contribute to a lack of bodily autonomy. Seek treatment providers who maximize personal responsibility and agency rather than those who seek to control your child’s behaviors.
Look for ways to improve your empathy, unconditional positive regard, and attunement to your child’s emotional needs. Seek support and guidance from a counselor, therapist, or coach to learn these skills.
Moving forward
If your child is in immediate medical danger, you may need to take control of their physical health. But you can still improve your child’s bodily autonomy through the process. Many parents have to make choices that impact their kids’ bodily autonomy. It’s OK! Just help your child process the trauma with the help of a trained trauma therapist.
Terri found a wonderful EMDR therapist for Natalia who worked with her medical trauma. Meanwhile, Terri worked on expanding Natalia’s sense of agency and control over her life. While she couldn’t release all oversight of Natalia’s health due to the eating disorder, we found lots of small ways to increase Natalia’s sense of freedom and choice in other areas of her life.
Recognizing the link between bodily autonomy and the psychology of eating disorders made a big difference. Within a few months, Terri felt closer and more connected to Natalia, and things were looking a whole lot better for the whole family!
Ginny Jones is the founder of More-Love.org, and a Parent Coach who helps parents who have kids with eating disorders.
For privacy, names and identifying details have been changed in this article.
At the heart of many eating disorders are toxic cognitive distortions: rigid, negative thought patterns that distort reality and feed harmful behaviors. These thoughts, like “I’m not good enough” or “I don’t deserve to eat,” can quietly take root, reinforcing shame, fear, and a desperate need for control. Understanding how these mental traps operate is key to breaking the cycle of disordered eating and beginning true healing. In this article, we’ll explore the most common cognitive distortions that fuel eating disorders and how to start challenging them.
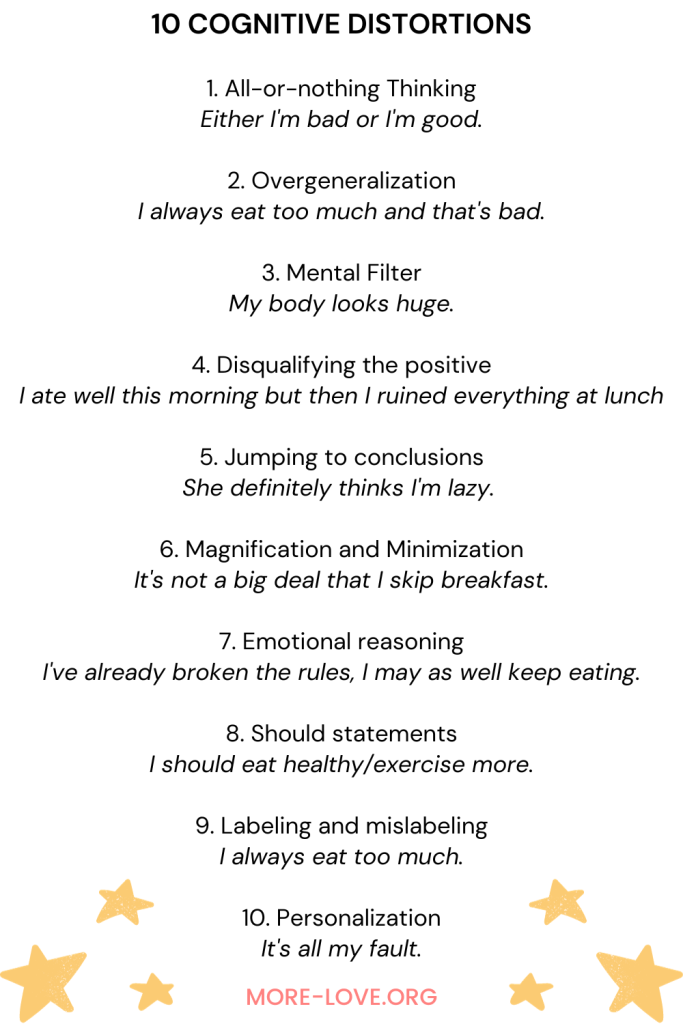
People who have eating disorders often exhibit 10 common cognitive distortions that are well known in psychology. Cognitive distortions are a hallmark of anxiety, depression, eating disorders, and many other mental disorders. The good news is that cognitive therapy is very effective, and parents can do a lot at home. Counteracting cognitive distortions can help people gradually replace distorted thinking with healthy, adaptive thinking.
The 10 cognitive distortions and eating disorders
The cognitive model was developed by Aaron Beck in the 1960s. The theory suggests that individuals’ perceptions of their experiences impact their emotional, behavioral, and physiological responses. By addressing and correcting these misperceptions, as well as modifying unhelpful thoughts and behaviors, individuals can experience improved reactions. This is the foundation of Cognitive Behavioral Therapy (CBT).
Cognitive distortions refer to negative or irrational thinking patterns that can have detrimental effects on motivation, self-esteem, and contribute to issues such as anxiety, depression, eating disorders, and substance abuse. Here are some examples of how the 10 cognitive distortions can impact an eating disorder. These are common eating disorder thoughts that are addressed during treatment.
1. All-or-nothing Thinking
Someone who has an eating disorder often has what is commonly called “black-or-white” thinking. Nothing in nature is only one way or another. We all exist in the gray areas in between.
Eating disorders are based on the concept that food and weight are black and white issues. For example, a child might think “I’m fat” if they have even an ounce of fat on their bodies. This is despite the fact that all bodies must have some fat in order to be alive. They think “I ate too much” if they have stomach fullness. But feelings of fullness and satiety are perfectly natural biological feedback. They think “sugar is bad” even though sugar is just a food and is part of a normal diet.
Try this: If you see your child suffering from all-or-nothing thinking, intentionally talk about the gray area. If you’re watching a TV show together and the characters believe there are only two options, talk about how there are always many options. Notice when you make statements that support all-or-nothing thinking and correct yourself out loud in front of your child. If your child shares all-or-nothing thinking like “if I start eating I’ll never stop,” respond with something like “I know it can feel that way, but I don’t think your only options are either eat nothing or eat everything. There’s so much space in between.”
2. Overgeneralization
Someone who has an eating disorder tends to take note of negative experiences. They conclude that if they happen once, they will happen over and over again.
For example, they may think “I always overeat, and that’s why I’m fat.” This is even if they barely eat anything most of the time and then, to compensate, occasionally binge eat. If they fail to meet an arbitrary weight goal, they think “I’m never going to lose weight and will be lonely and miserable my whole life.” Overgeneralization feels like the absolute truth. This is despite the fact that many people may tell them in specific terms that they are incorrect.
Try this: Notice when people make sweeping statements that overgeneralize the human experience. For example, if you’re talking about a neighbor who “never mows his lawn,” correct yourself and say “actually, that’s not true. He mows it, but just not as frequently as I’d like him to. If your child makes an overgeneralization like “Nobody recovers from eating disorders,” say something like “I know it can seem like an impossible task, but lots of people do recover.”
3. Mental Filter
When a child has an eating disorder, they tend to create an inaccurate mental filter of how they appear and who they are. They see themselves as if through a distorted fun-house mirror.
This is seen in body dysmorphia, which commonly occurs with eating disorders. They literally see their bodies in a way that they do not exist. They may see bulges and bumps that are not there to any but their own eyes. Over time, they find it almost impossible to view themselves in any other way. This happens even when others objectively and authoritatively tell them that they are incorrect.
Try this: The next time your child tells you their body is imperfect, don’t automatically tell them they are beautiful and perfect. Instead, let them know that you understand they see a distorted view in the mirror. Just like those warnings on car mirrors, “objects in mirror are closer than they appear,” the mirror is not an accurate representation of reality. If they are struggling to see themselves, tell them that you see their beauty – inside and out – and will hold that for them until they can do the same.
⭐⭐⭐⭐⭐
Free Guide: How Parents Can Help A Child With An Eating Disorder
Master the secrets to supporting a child with an eating disorder. Thousands of families like yours are stronger today because of these six vital lessons drawn from lived experience, best practices, and extensive study.
People who have an eating disorder have an amazing ability to take neutral or positive feedback and turn it into something that reflects negatively upon themselves.
For example, if someone tells them they look nice, they may say they gained weight. If someone tells them they’ve lost weight, they may say that it’s not enough – they still have more to go. If someone tells them they are a healthy eater, they tell them they are far from perfect and need to be better.
This becomes compulsive. They are unable to accept a neutral or positive comment without washing it away with something self-deprecating. The belief behind the disqualification is typically some “fatal flaw” or belief of being “less than.”
Try this: Rather than debate with your child when they disqualify the positive in themselves, let them know that you see it. You don’t have to convince them of their positive elements, but you can tell them that you hold them in your heart and mind. Tell them your vision of them is multifaceted and dynamic, and you will continue to hold that no matter what they say or do.
5. Jumping to conclusions
Many who have eating disorders believe they can read other people’s minds, especially when it comes to negative feelings towards themselves. They may “know” that someone thinks they’re fat and ugly, stupid and lazy, or any other negative belief.
Their mind-reading efforts are almost limitless. They will read the minds of people who are actually not even aware of their presence. And they can obsess about what a person who passed them in a hallway was thinking about them even when the other person actually had no thoughts at all! Sometimes they take mind-reading to epic proportions and confront people about their supposed thoughts with no evidence.
This can have disastrous effects and result in a self-fulfilling prophecy. They begin to shape the way people see them.
Try this: Listen for when your child jumps to conclusions about what other people think and believe. Say “I can understand why you think that, but I also believe we can’t read other people’s minds. Often when we think one thing, it turns out that we are wrong.” You don’t need to get into a debate about the validity of what you’ve just said. That will only weaken its power. Just let it stand.
6. Magnification and Minimization
This is a habit in which a person who has an eating disorder magnifies their perceived flaws while simultaneously minimizing the idea that there is a problem with how they perceive themselves.
For example, they may think “I’m so disgusting, nobody will ever love me, and I’m going to be sad and alone forever.” If they actually say this out loud, a loved one may become concerned and urge them to seek treatment.
At that point, they will switch to minimizing the problem. They may say “everyone feels like this, I’m nothing special. Life is just hard.” Minimization is partly how they deny the severity of an eating disorder. It gives them the belief that they are not sick enough to warrant treatment.
Try this: It’s important for parents to neither over- nor under-react to these situations. The more you can stay steady and calm in the face of magnification and minimization, the greater your chances of showing your child that there is always a middle ground. No, they may not be the sickest person ever, but they may still have some concerning behaviors that you believe deserve care and attention.
7. Emotional reasoning
When a person has an eating disorder, they take their emotions and emotional thoughts as evidence of the “truth.” This means that if they think they are fat, they must be fat. If they think they eat too much, they must eat too much.
This can also be seen in binge eating mentality, which can begin with “I’ve already broken the rules, I may as well keep eating.” Emotional reasoning is dangerous because thoughts and beliefs are not usually facts. In fact, usually the first, easiest thought that comes to mind is a societally-driven, conditioned thought.
This is classically experienced as “I feel fat.” In our society, “fat” is a euphemism for any number of emotions. These emotions include depressed, lonely, sad, angry, scared, etc. When someone gets stuck in emotional reasoning, they forget to look deeper at their thoughts. They take them at face value rather than utilizing them as signals pointing them towards what is really upsetting.
Try this: Talk to your child about the idea of having a first thought and a second thought. The first thought is a knee-jerk reaction based on our societal conditioning. We need to tap into our conscious thought and look for the second thought, which is almost always much more nuanced and realistic.
8. Should statements
Maintaining an eating disorder is often based on “shoulds.” The most common shoulds are “I should lose weight,” and “I should eat healthy/exercise more.” These shoulds come directly from our society. They are reinforced in almost every aspect of life until they become so pronounced that people notice them as the problematic beliefs they are.
The trouble with should statements is the shame that accompanies them. People inevitably break their shoulds. Our behavior will inevitably fall short of our expectations when we are should-ing all over ourselves.
When a person succeeds in meeting their shoulds, they may feel a temporary sense of self-righteousness. But this is always followed by the terrible fall into bitterness and shame when they inevitably fail something else.
Try this: When your child says “should,” gently remind them that they always have options, and there is rarely a single right solution to any problem. Encourage them to think more deeply about why they believe they “should” do something and help them loosen up those beliefs that are holding them hostage.
9. Labeling and mislabeling
The deeper a person gets into an eating disorder, the more they feel they need to label ourselves, and ultimately it comes down to whether they are “good” or “bad.”
They don’t say “I ate a big meal at lunch today.” Instead they say “I always eat too much.” They don’t say “I carry my body weight in my hips.” Instead they say “My hips are huge.”
These big labels help them feel we have some measure of control over their bodies. This is a false belief because except in very extreme cases our bodies will find a way to achieve the genetic blueprint that largely determines our weight and shape.
A person who has an eating disorder often mixes up who they are as a person with how they appear in their body. A person is not a body – we is infinitely more flexible, adaptable, and interesting. When we define ourselves based on our bodies, we suffer tremendously and deny the world of a bright mind and unique self.
Try this: When your child labels their whole self as some version of “good” or “bad,” talk to them about the idea of “parts of self.” All of us are multifaceted and dynamic. We are not a single monolithic being that can be labeled. If your child says “I’m angry,” say “it sounds like there’s a part of you that is angry right now.” This is a crucial reframing that takes them from a monolithic view to a parts-based, temporary view.
⭐⭐⭐⭐⭐
Free Guide: How Parents Can Help A Child With An Eating Disorder
Master the secrets to supporting a child with an eating disorder. Thousands of families like yours are stronger today because of these six vital lessons drawn from lived experience, best practices, and extensive study.
Many people who have eating disorders take things very personally. They believe that they are personally responsible for other people’s feelings and actions. This means they carry a heavy emotional load that does not help anybody.
Personalization is a terrible situation in which a person gets stuck pointing our fingers at themself, no matter what happens. If they don’t lose weight because their body’s metabolism slowed down, it’s their fault. They also believe that the size of their bodies is responsible for how other people feel.
They may believe that if they maintain a thin body, their parents will feel good and other people will like them more.
Of course, this is not true. If people have any feelings about the weight of another person’s body, that is because they have weight stigma. It has nothing to do with the other person’s body, and everything to do with them. Other people are completely responsible for their own choices, beliefs, and behaviors. While we have influence in relationships, we are never responsible for another person’s feelings.
Try this: Remind your child that they are not personally responsible for anyone’s feelings and behavior except their own. When other people behave badly, that is their reaction to external factors. We do not control other people’s reactions. It’s important to model this in your parent-child relationship. Instead of saying “you make me so mad!” say “I’m feeling very mad right now, and I need a minute to settle myself down.” This way you show them that you are responsible for your feelings and for responding to them appropriately.
Parents can help reduce cognitive distortions
While food and weight issues are the symptoms, cognitive distortions are part of the psychology of eating disorders. The eating disorder behavior is an attempt to manage the cognitive distortions. When parents know to look behind the behaviors to the root causes, they can help their child recover. The more we understand and tend to our child’s emotional health, the better.
FAQs about cognitive distortions and eating disorders
What does “cognitive” mean?
Cognition is defined as thinking, knowing, remembering, judging, and problem-solving.
What are “cognitions”
Cognitions are typically defined as thoughts, beliefs, judgments, and opinions.
What is a “cognitive distortion?”
Cognitive distortions are often distorted thoughts and thinking patterns that get in the way of feeling good about oneself and others.
How are cognitive distortions related to eating disorders?
Cognitive distortions both cause eating disorders and are a symptom of an eating disorder. That’s why changing cognitive distortions is a key part of treating eating disorders. There are 10 cognitive distortions that often lie beneath the surface of eating disorder behaviors. These cognitive distortions may linger after eating disorders have otherwise receded. It is a good idea to be aware of these cognitive distortions and continue your child’s therapy as long as these distortions are present.
What are the most common cognitive distortions with an eating disorder?
Common cognitive distortions for people with an eating disorder include believing that they have to be thin to be loved, that losing weight is a requirement of being accepted, and that controlling food and weight will result in a better life. With these cognitions in place, a person might use eating disorder behaviors like food restriction, over-exercise, and purging. These behaviors will lead to binge eating for some, but not others.
Ginny Jones is the founder of More-Love.org, and a Parent Coach who helps parents who have kids with eating disorders.
Many people who have eating disorders like anorexia, bulimia, binge eating disorder, and ARFID also have ADHD, autism, OCD, and/or PTSD. These conditions are commonly found together and can make treatment harder if they’re not addressed in relationship to each other.
My client Crystal was stunned when, three years into treatment, she found out that her daughter had PTSD and autism that pre-dated the eating disorder symptoms.
“We started treatment three years ago for the eating disorder before we even knew about the PTSD,” says Crystal. “I remember getting so frustrated with my daughter’s treatment team because they kept asking probing questions about trauma and we were convinced that had nothing to do with her eating patterns. I was sure the problem started and ended with her desire to look like an Instagram influencer, but I was wrong.”
Crystal isn’t the only one who’s been led astray by the common misunderstanding that eating disorders are skin-deep. That they’re about an obsession with physical appearance. Of course, negative body image is a major symptom of an eating disorder. But eating disorders don’t only come from the false body ideals presented by the media, otherwise, 100% of people would have eating disorders.
In recent years we’ve come to understand that eating disorders rarely show up alone, and they’re much more than skin-deep. They’re often a complex coping mechanism for other neurobiological conditions and mental disorders. The intersection of conditions like ADHD or autism and an eating disorder must be addressed holistically for treatment to be effective.
Eating disorders can be a coping mechanism
It’s easy to miss the underlying drivers of an eating disorder. Often we’re distracted by the belief that eating disorders are about looking a certain way and meeting societal standards. And of course, that’s a part of it. However, the drive to achieve societal standards can be considered a symptom of the eating disorder. The root cause of the eating disorder may be underlying neurobiological and mental conditions. These conditions make your child sensitive to disordered eating patterns in the first place.
In many cases, eating disorder behaviors are a sort of secondary condition that lies on top of disorders like ADHD, OCD, PTSD, and/or autism.
As a parent who has a child with an eating disorder, you need to understand that it’s possible your child’s disorder goes much deeper than food, eating, and weight, and includes an underlying condition. If you know your child has an eating disorder alongside something like autism or ADHD, ask their treatment team specifically how they are addressing eating behaviors within the context of treating the other condition. They should have a strong answer for you, as these conditions can’t be treated in isolation!
If your child’s only condition right now is an eating disorder, explore whether something else might be driving their symptoms. Ask their treatment team if they’ve been evaluated for ADHD, autism, OCD, and/or PTSD. Both ADHD and autism are chronically underdiagnosed in females, which also happens to be the population at the highest risk of an eating disorder. Finding out if your child has ADHD or autism might not be something you were looking for, but when an eating disorder is present it should be explored.
Obsessive Compulsive Disorder
Obsessive Compulsive Disorder (OCD) falls under Anxiety Disorders, and both Anxiety Disorders and OCD are highly correlated with eating disorders. A research study in 2004 found that 64% of people who have eating disorders also suffer from an anxiety disorder. And up to 41% have OCD in particular. The study also found that 42% developed anxiety disorders in childhood before the eating disorders began. (ADAA)
Some researchers even place eating disorders under the umbrella of OCD rather than stand-alone disorders. This causes some real challenges when treating someone with an eating disorder. This is because the clinician may not be clear about where one disorder ends and the other begins. (IOCDF)
Eating and weight obsessions
Most of us think of OCD as being about obsessively washing hands. But weight and food obsessions, body checking, and eating rituals fall well within the spectrum of OCD. Many people who have eating disorders have obsessive and compulsive thoughts about food and weight.
People who have eating disorders may use restriction, purging, and/or binge eating as a way to manage feelings of anxiety. Anxiety is often described as the persistent sense that something is terribly wrong. Some experience heart palpitations, stomach upset, and trouble breathing. Others faint when facing especially stressful situations. It’s very common to think an anxiety attack is a near-death experience. The physical sensations of fear are as pervasive and terrifying as being chased by a lion.
Working with both OCD and an eating disorder involves a combination of therapies. Most professionals who work with OCD use exposure therapy. They may also use Cognitive Behavioral Therapy (CBT) and/or Dialectical Behavioral Therapy (DBT). Both are highly effective in treating Anxiety Disorders. If your child has OCD they will likely require ongoing mental health support beyond eating disorder recovery.
A program called SPACE is highly effective in reducing symptoms of anxiety, eating issues, and OCD. SPACE teaches parents how to respond more effectively to anxiety. Studies show that teaching parents these skills is as effective as working with the child using CBT.
ADHD
Several studies have found a link between ADHD and eating disorders, particularly bulimia. The working theory on why this happens is that impulsivity is recognized as a trait for both conditions. The treatment for an eating disorder is distinctly different from and may even contradict the treatment for ADHD. This is why both conditions must be considered in treatment.
For example, treatment may begin either with managing the symptoms of ADHD or managing the symptoms of the eating disorder. Often the choice is made based on the experience of the team and the severity of the symptoms. ADHD is frequently missed in girls. Thus, this underlying condition is often missed in female eating disorder treatment.
One study found that for girls, ADHD significantly increases the risk of eating disorders. They showed a particular risk of developing bulimia nervosa. Girls with ADHD and an eating disorder had increased rates of mood, anxiety, and disruptive behavior disorders.
Additionally, ADHD traits are highly predictive of the severity of anxiety and depression symptoms, both precursors and companions to eating disorders. The higher the levels of ADHD traits, the more likely a person is to experience severe mental health symptoms. Due to societal biases and misinformation, people with ADHD often don’t receive access to the clinical care they need to cope with their symptoms. Importantly, ADHD isn’t just a childhood condition that people “grow out of,” but persists throughout life.
One of the most commonly reported relationships between ADHD and eating disorders is the issue of eating regularly. ADHD often interferes with planning and regularity. Therefore skipped meals can become a problem, resulting in binge eating later in the day. It can be hard to tease apart the two issues, but doing so can greatly improve treatment efficacy.
Autism
Research has found links between Autism Spectrum Disorder (ASD) and Anorexia Nervosa. (Eating Disorder HOPE) People with autism often exhibit repetitive behaviors and restrictive behaviors and interests. They also can have sensory sensitivities.
Atypical eating behaviors, including limited food preferences and hypersensitivity to texture, are found in 70.4% of children with autism. This figure is so high that it has been suggested that atypical eating behaviors may be used as a diagnostic tool for autism. Feeding problems, such as picky eating, fear of trying new foods, food avoidance, and insistence on specific food presentation are common in youth with autism.
These atypical eating behaviors may explain why between 20-30% of people with eating disorders also have autism or signs of autism. Autism is especially correlated with ARFID (Avoidant Restrictive Food Intake Disorder). There is even a hypothesis that underdiagnosis and subsequent lack of treatment for autism may mean that many girls diagnosed with anorexia have a primary condition of autism.
The diagnostic tests for autism lean heavily towards boys – more than four boys are diagnosed for every one girl. While there may be genetic differences, clinicians are now considering that there is a gender bias in the diagnostics and autistic girls are less likely to be tested and diagnosed. These girls don’t fit the stereotypes or their symptoms are misinterpreted. Additionally, girls may be better at “masking” their autistic traits. Some say that under-diagnosis and subsequent lack of treatment may mean that many girls with anorexia are suffering from ASD.
One symptom of Autism is the ability to hyperfocus. This may translate into extensive rituals around logging calories and body weight as seen in someone who has anorexia. The continued hyperfocus even when other people suggest relaxing food rules can also be seen as a symptom of ASD.
Another symptom of Autism is being highly sensitive. Many people who have ARFID have a strong aversion to specific food textures, smells, and even colors. Some will talk about the discomfort they feel when chewing, swallowing, and digesting food. This could suggest high sensitivity in the mouth, throat, and digestive tract.
These overlapping symptoms can make it hard to tease apart ARFID from anorexia. The term Avoidant/Restrictive Food Intake Disorder (ARFID) is now used to differentiate people who restrict food for non-weight reasons. Meanwhile, anorexia is a disorder in which the active pursuit is low body weight.
The SPACE-ARFID program has been developed specifically to address non-weight-based food restrictions. It’s been found to be highly effective in reducing food and eating anxiety and increasing food and eating flexibility.
Post Traumatic Stress Disorder
People who have eating disorders have a higher rate of childhood trauma compared to the general population. Sexual trauma seems to be particularly linked to eating disorders. Women who have a history of childhood sexual abuse are more likely to have problematic eating behaviors and eating disorders. Trauma includes physical and emotional violence, sexual abuse, emotional neglect, having a serious accident or illness, witnessing a serious accident or illness, and more. A relatively new form of trauma being explored is complex trauma. This is the trauma a child experiences when their attachment needs with caregivers are not adequately and consistently met.
Symptoms of trauma include emotional dysregulation, a negative self-image, and the inability to cope with strong feelings such as anger or sadness. Experts have suggested that people who have a history of trauma may develop eating disorders as a way to cope with their trauma since eating disorder behaviors can be powerful self-soothing and coping mechanisms.
Most of us think of soldiers returning from war when we hear about PTSD. But the disorder is found in 10% of women and 4% of men. The higher prevalence of PTSD in women is likely because they are more likely to experience sexual assault. Such a violation is more likely to cause PTSD than many other types of events. The most common trauma for women is sexual assault or childhood sexual abuse. About 33% of women experience sexual assault during their lives, many before they reach adulthood. (National Center for PTSD)
Trauma rewires the brain
Trauma rewires the brain and nervous system. It results in chronically increased stress hormones and reduces the ability of the brain to communicate with the body. People suffering from PTSD may confuse fear and pain with pleasure. They will commonly push their bodies beyond reasonable boundaries. This includes extreme restriction, binge eating, self-harm, substance abuse, over-exercising, and extreme risk-taking (The Body Keeps the Score). One study found that +33% of individuals who have PTSD are still suffering from the full syndrome a decade later. In other words, it is frequently undiagnosed and undertreated.
It has been suggested that Bulimia Nervosa, in particular, may emerge as a coping method for the pain of PTSD. Women who have anorexia exhibit standard rates of PTSD (10%). However, about 25% of women with Bulimia Nervosa are diagnosed with PTSD. (Eating Disorder HOPE)
If you suspect that one of these diagnoses may be contributing to your child’s eating disorder, ask their treatment team whether they have been assessed. If not, you can request testing for any of these psychological conditions.
Ginny Jones is the founder of More-Love.org, and a Parent Coach who helps parents who have kids with eating disorders.
Experiencing sexual trauma and struggling with an eating disorder can create a complex and deeply painful journey toward healing. These challenges often intertwine, with trauma impacting one’s relationship with food, body image, and self-worth.
Coping with both requires understanding, patience, and specialized support that addresses the unique ways trauma influences eating behaviors. In this article, we’ll explore effective strategies to manage the dual impact of sexual trauma and eating disorders, offering hope and guidance for survivors seeking recovery and resilience.
One study found that 1 in 6 teen girls was harassed in the last six months. One in 5 girls between 14 and 18 years old reported being sexually assaulted. And 6% of girls surveyed said they had been raped. Another survey found that 48% of 7-12 graders experienced sexual harassment during the 2010-2011 school year.
A social crisis
We know that women are more likely to develop eating disorders in our culture. And we know there is tremendous pressure for girls and women to pursue beauty and thinness. But that doesn’t tell the full story. Women in our culture are frequently harassed and abused simply for their gender. And few speak of it due to the fear of retribution. We also have a very low rate of action against people who are accused of sexual crimes.
*Quick note: I know that boys are both sexually traumatized and develop eating disorders. In this article, I’m focusing on girls, but the advice holds true for any gender.
No matter how good our parenting is, we can’t control the social situations our child enters. Schools, church groups, sports teams, and all social settings can be places where our girls may be sexually targeted.
Our culture does not currently hold sexual abusers accountable for their actions. Nor do we train people to not become sexual abusers. Until that happens, we must take steps to help our daughters recognize and address sexual harassment, assault, and rape. We must provide them with knowledge and tools that they can use to protect themselves from sexual harassment whenever possible. If the worst happens, we must intervene quickly and aggressively.
What is sexual trauma?
Sexual trauma is usually caused by sexual harassment, assault, or rape.
Sexual harassment may include making comments about a person’s appearance, body parts, sexual orientation, or sexual activity. These comments may be said out loud, performed using gestures, or written using texts or social media. Their intention is to hurt, offend or intimidate another person. Regardless of how they are communicated, they are always inappropriate and need to be addressed.
Sexual harassment turns into assault when it gets physical. This is when someone tries to kiss or touch someone who doesn’t want it. Rape is when a person forces someone else to have sex with them.
Given the statistics, it’s not uncommon for parents to have been sexually harassed, assaulted, and even raped in the past. This may make them hesitant to treat sexual trauma too seriously. They may have developed a coping mechanism of downplaying the impact of their own sexual trauma. But it’s important to know that our girls need protection against and action when sexual trauma occurs. Every person deserves to have sovereignty over their body.
Eating disorders and sexual trauma
Sexual trauma is associated with the development of eating disorders. There are many reasons for eating disorders. But traumatic experiences, especially those involving the body, are some of the most strongly correlated event-based triggers for eating disorders.
Alisa was 12 when she was sexually assaulted by some boys from school. She thought they were friends, but one night their sexual innuendos crossed the line. Alisa froze and felt trapped and afraid about what would happen next. She didn’t feel like she could tell anyone. Even though she was close to her parents, she felt ashamed of what had happened. She felt that it was her fault because she flirted back in the beginning.
Alisa became increasingly anxious, which decreased her appetite. She found it more and more difficult to eat. By the time her parents became aware, she was deep into an eating disorder. She refused almost all foods except a few that she had identified as safe.
Her parents got her into treatment and her care team uncovered the assault. Once they knew about it, they were able to work with Alisa on processing her trauma. Her parents pursued reformative justice for the boys involved. With her parents’ support and care, she began to heal.
What parents can do about sexual trauma and eating disorders
Eating disorders arise when a person’s body feels unsafe. This means that sexual trauma can be a trigger. The thing that really needs to happen is for people to be trained to NOT sexually traumatize others. But we live in a society in which sexual trauma frequently occurs with very few consequences. Therefore, we need to raise our girls to identify and speak out against sexual harassment, assault, and rape.
1. Talk about boundaries
Have frequent conversations with your daughter about sexual boundaries. Sexual harassment often begins with a small innuendo or joke, which she may not know how to handle. Help her build some language for responding to jokes, even from friends. Discuss the three levels of sexual abuse: harassment; assault; and rape. Talk to your daughter about consent. Remind her that she has the right to say no when someone tries to violate her boundaries. This stays true regardless of her relationship status, behavior, dress style, or past history.
2. Pay attention to school, work, sports, and church groups
Talk to your daughter about who she is in contact with on a daily basis. Does she feel comfortable with her peers and adults involved in the activities she’s involved in? Pay attention to any abrupt changes in her willingness to attend places and events. Especially if they were previously comfortable, fun places for her. Ask whether something happened and whether there is anything you can do to help. Remember that she may not be able to talk to you with words. But her behavior may show you there is a problem.
3. Set digital boundaries
Text groups and social media apps can be filled with sexual innuendo and harassment. Group conversations can go from fun to dangerous very quickly. Talk to your daughter about what is and what is not acceptable in digital media. For example, taking photographs of body parts, discussing body parts, and other sexualized activities online should be strongly discouraged. Determine whether you need to monitor conversations. This may be necessary to support your daughter as she learns to identify sexual harassment situations.
4. Report problems immediately
Don’t hesitate to discuss sexual harassment with your daughter’s school, sports team, church, etc. There is a good chance that your child will not be comfortable doing this herself. And this is a time when she needs your active participation as a parent. Don’t let her, or anyone else, tell you to just “let it go.” Be persistent in following your complaint through the system. And engage an attorney specializing in sexual harassment if necessary. Your rigorous defense of her body is critical to her sense of safety and healing.
5. Get treatment for your child
Many girls find themselves living with PTSD following sexual trauma situations. Don’t wait for signs of distress. If your daughter has sexual trauma, schedule an appointment with a qualified therapist. She will likely need help processing what happened. Even if she is not traumatized by the event, she may find herself traumatized by the aftermath. Reporting someone for sexual crimes is extremely stressful in our society, and she will need support in handling the fallout.
6. Continue to watch for signs of distress
Many times, victims of sexual trauma go months – even years – before the impact of the trauma makes itself known. A delayed response to a traumatic event is common. In fact, many survivors forget it happened to protect themselves. This is where behaviors might be your best sign that there is something wrong. Numbing behaviors like substance abuse, self-harm, suicidality, and eating disorders may be symptoms of PTSD. Be vigilant in continuing the conversation with your child. And watch for psychological signs of distress so that you can help your child heal from the trauma, no matter when it presents itself.
Ginny Jones is the founder of More-Love.org, and a Parent Coach who helps parents who have kids with eating disorders.
Eating disorders often develop as maladaptive coping behaviors, ways individuals try to manage overwhelming emotions, stress, or trauma that feel unmanageable otherwise. Understanding these coping mechanisms is crucial for recognizing the deeper struggles behind disordered eating and providing effective support.
Maladaptive behaviors might include restrictive eating, bingeing, purging, or excessive exercise, all serving as unhealthy tools to cope with pain or anxiety. In this article, we’ll explore how these behaviors connect to eating disorders and offer insights to help parents help their children move toward healthier coping strategies and healing.
What is a maladaptive coping behavior?
A maladaptive coping behavior is a behavior that we utilize to soothe ourselves when we feel anxious.Mildly avoidant coping behaviors may look like frequently avoiding using the elevator because you feel a bit anxious in elevators and stairs are easily accessible.
But sometimes coping behaviors can overwhelm our ability to live a “normal” life. For example, a fear of elevators may mean refusing to ever ride in an elevator, spending excessive energy and time researching stair access in buildings, using the stairs even when it adds significant hardship, and refusing to go places that don’t have reasonable stair access (e.g. an office on Floor 10 or above). At this point, when a coping behavior interferes with normal life, it may be called “maladaptive.”
It’s important to note that maladaptive coping behaviors start out as a good solution to an emotional problem. But when they interfere with life they become disordered. Nobody is “bad” for having a maladaptive coping behavior. But we do have ways of treating maladaptive coping behaviors, also known as disordered behaviors. This is what recovery is. Even them most deeply-entrenched maladaptive coping behaviors can be overcome, but it takes tremendous effort and support. The most-recognized method for recovering from maladaptive coping behaviors is to build emotional regulation skills and healthy coping strategies.
Maladaptive coping behaviors are a response to anxiety
Maladaptive coping behaviors usually start small, such as avoiding the elevator when it’s convenient. But they can also grow over time and take over our lives. This is because the problem is rooted in anxiety. Anxiety impacts us both psychologically and physically. Some symptoms of anxiety include:
Racing thoughts
Uncontrollable fear
Rage
Asking the same question over and over again
Wanting to run away
Extreme chest pain
Crying or screaming
Jittering or shaking
Nausea or heartburn
Fainting or physically shutting down
Obviously, when we feel these awful symptoms of anxiety, we want them to stop. We need them to go away! So we reach for coping behaviors to feel better. Coping mechanisms can be mild or severe. They typically make us feel better temporarily, but increase anxiety and maladaptive coping in the long run.
Maladaptive coping behaviors help in the short term but hurt in the long term. They may have physical, emotional, and social side effects that are even worse than the anxiety itself. They also tend to make anxiety get worse over time. Healthy coping behaviors will help in the short- and long-term, and they reduce anxiety over time.
⭐⭐⭐⭐⭐
Free Guide: How Parents Can Help A Child With An Eating Disorder
Master the secrets to supporting a child with an eating disorder. Thousands of families like yours are stronger today because of these six vital lessons drawn from lived experience, best practices, and extensive study.
Anxiety disorders are common, and thus maladaptive coping behaviors are also fairly common. Some maladaptive coping behaviors include:
Eating disorders
Shoplifting/Kleptomania
Overspending/Shopping addiction
Promiscuous sex/Sex addiction
Substance abuse/Alcohol abuse
Self-harm
Compulsive lying
It is very common for a person to develop more than one maladaptive coping behavior or mechanism. Another thing that often happens is we will overcome one maladaptive coping behavior only to replace it with a different one. For example, someone who had an eating disorder may develop a substance abuse problem.
What’s the reason for maladaptive coping behaviors?
At their core, maladaptive coping behaviors like eating disorders are attempting to help us. They seem like a great idea because they immediately seem to solve a distressing emotional state.
Here are some examples of people using maladaptive coping behaviors:
Jane feels stressed and unloved when she visits with family. After family events, phone calls, and even emails she shops compulsively and has racked up thousands of dollars in credit card debt.
Michael divorced his partner and feels lonely. Every night he comes home to an empty house and eats bags of potato chips and cartons of ice cream, then gets a stomachache and feels ashamed of himself for having no control.
Sarah suffered sexual trauma as a child and now has PTSD. Several nights each week she finds herself at bars picking up on strangers and sleeping with them. She wishes she wouldn’t do this, and doesn’t understand why it keeps happening.
Jamal’s parents were both incarcerated and used substances heavily. He always swore that he wouldn’t get mixed up in that and became a successful lawyer with a family. But he has fallen into the habit of drinking a bottle of wine every night, sometimes more.
Maladaptive coping behaviors are rarely something that we “pick” or decide to do. They typically arise from our subconscious and feel compulsive and instinctual. They usually feel like the only option to living life with anxiety.
When a behavior becomes maladaptive
Most people can relate to at least one of the coping behaviors we listed. That’s because everyone uses coping behaviors, and they aren’t always maladaptive. For example, most people have used shopping, alcohol, food, and other maladaptive coping behaviors occasionally to cope with stress.
It’s important to recognize the difference between using something occasionally and feeling better and using something compulsively. A person who is stuck in a maladaptive coping behavior may notice that they feel:
Compelled to use the behavior even if they don’t want to
Ashamed of themselves for using the behavior
Notice that they need the behavior more often and/or need a higher dose over time
These three elements can signal that someone is becoming dependent on a maladaptive coping behavior.
How can we stop maladaptive coping behaviors?
The most important thing to recognize when dealing with maladaptive coping mechanisms is that they are there to help. While they may look obviously destructive to other people, the person who is using them feels soothed and better when using the behavior.
This is why saying that someone needs to stop the maladaptive coping behavior “cold turkey” can backfire. Unless we replace the maladaptive coping behavior with healthy coping behaviors, we can cause more harm than good.
If we want a child or someone we love to stop using maladaptive coping behaviors like eating disorders, we need to help them uncover the stress they are trying to cope with. Then we need to help them build healthy coping behaviors so they can replace one with the other.
If we try to rip the maladaptive coping behavior away without recognizing the purpose the behavior is serving, we risk driving it underground or morphing into another form because we have not actually addressed the core problem.
Actively seeking care and attention from loved ones
Developing some distraction “tricks” to get through an anxious state, such as making a list of fruits and vegetables, naming all of the car manufacturers, or seeking a specific color in the environment.
Reaching out to a friend or family member for help
Getting professional therapy, counseling, or coaching
Participating in and feeling as if you belong to a community
We created this short video to illustrate maladaptive coping mechanisms.
How we feel feelings
When we are in a normal state, various feelings circulate in and out of our minds rapidly. However, when we have depression or anxiety, our feelings begin to get stuck in our orbit. Then, negative feelings become larger, while positive feelings become smaller.
At this point, some of us engage maladaptive coping mechanisms in an attempt to protect ourselves from these negative emotions. Unfortunately, when we use these coping mechanisms, we minimize and keep out positive emotions even more than before.
Feeling better in the short-term
Maladaptive coping mechanisms are behaviors that make us feel better in the short term, but in the long-term, they are very harmful. They are part of the psychology of eating disorders, self-harm, alcohol & substance abuse, sexual promiscuity, shoplifting, risk-taking behavior and compulsive lying.
Once we become dependent on our maladaptive coping mechanisms, we become emotionally weaker, and even less able to withstand negative emotions. But our maladaptive coping mechanisms convince us that they are the solution to our pain.
Even as our maladaptive coping mechanisms bring us to our knees, we are unable to see how they are perpetuating the pain we are trying to avoid.
⭐⭐⭐⭐⭐
Free Guide: How Parents Can Help A Child With An Eating Disorder
Master the secrets to supporting a child with an eating disorder. Thousands of families like yours are stronger today because of these six vital lessons drawn from lived experience, best practices, and extensive study.
Adaptive, or healthy coping mechanisms, are skills that we must learn in order to overcome our maladaptive coping mechanisms. If we try to stop our maladaptive behavior without learning healthy skills, we are unlikely to succeed. Healthy coping skills include learning to process emotions, learning to care for ourselves, and being assertive about our needs.
As we slowly learn these skills, we gain strength against the maladaptive coping behavior, slowly integrating our new tools for managing negative emotions. As we do this, positive feelings become more present in our lives. Over time, our feelings begin to circulate again. Even as this happens, and even as we begin to feel positive emotions again, we must be vigilant about practicing our healthy skills to ensure we can make a full transition and become truly recovered.
Recovery from maladaptive coping behaviors
People can and do recover from maladaptive coping behaviors like eating disorders. The key is to learn to “urge surf” or allow the urge to arise but respond with adaptive coping mechanisms.
Recovery means that we can live in the world and experience a broad variety of positive and negative emotions. We no longer need to rely on our maladaptive coping behavior to feel safe and secure.
Ginny Jones is the founder of More-Love.org, and a Parent Coach who helps parents who have kids with eating disorders.
We use cookies to improve your experience on our site. By using our site, you consent to cookies.
This website uses cookies
Websites store cookies to enhance functionality and personalize your experience. You can manage your preferences, but blocking some cookies may impact site performance and services.
Essential cookies enable basic functions and are necessary for the proper function of the website.
Name
Description
Duration
Cookie Preferences
This cookie is used to store the user's cookie consent preferences.
30 days
These cookies are needed for adding comments on this website.
Name
Description
Duration
comment_author
Used to track the user across multiple sessions.
Session
comment_author_email
Used to track the user across multiple sessions.
Session
comment_author_url
Used to track the user across multiple sessions.
Session
Google reCAPTCHA helps protect websites from spam and abuse by verifying user interactions through challenges.
Name
Description
Duration
_GRECAPTCHA
Google reCAPTCHA sets a necessary cookie (_GRECAPTCHA) when executed for the purpose of providing its risk analysis.
179 days
Statistics cookies collect information anonymously. This information helps us understand how visitors use our website.
Google Analytics is a powerful tool that tracks and analyzes website traffic for informed marketing decisions.
Used to distinguish new sessions and visits. This cookie is set when the GA.js javascript library is loaded and there is no existing __utmb cookie. The cookie is updated every time data is sent to the Google Analytics server.
30 minutes after last activity
__utmc
Used only with old Urchin versions of Google Analytics and not with GA.js. Was used to distinguish between new sessions and visits at the end of a session.
End of session (browser)
__utmz
Contains information about the traffic source or campaign that directed user to the website. The cookie is set when the GA.js javascript is loaded and updated when data is sent to the Google Anaytics server
6 months after last activity
__utmv
Contains custom information set by the web developer via the _setCustomVar method in Google Analytics. This cookie is updated every time new data is sent to the Google Analytics server.
2 years after last activity
__utmx
Used to determine whether a user is included in an A / B or Multivariate test.
18 months
_ga
ID used to identify users
2 years
_gali
Used by Google Analytics to determine which links on a page are being clicked
30 seconds
_ga_
ID used to identify users
2 years
_gid
ID used to identify users for 24 hours after last activity
24 hours
_gat
Used to monitor number of Google Analytics server requests when using Google Tag Manager
1 minute
_gac_
Contains information related to marketing campaigns of the user. These are shared with Google AdWords / Google Ads when the Google Ads and Google Analytics accounts are linked together.
90 days
__utma
ID used to identify users and sessions
2 years after last activity
__utmt
Used to monitor number of Google Analytics server requests
10 minutes
SourceBuster is used by WooCommerce for order attribution based on user source.
Name
Description
Duration
sbjs_migrations
Technical data to help with migrations between different versions of the tracking feature
session
sbjs_session
The number of page views in this session and the current page path
30 minutes
sbjs_udata
Information about the visitor’s user agent, such as IP, the browser, and the device type
session
sbjs_first
Traffic origin information for the visitor’s first visit to your store (only applicable if the visitor returns before the session expires)
session
sbjs_current
Traffic origin information for the visitor’s current visit to your store
session
sbjs_first_add
Timestamp, referring URL, and entry page for your visitor’s first visit to your store (only applicable if the visitor returns before the session expires)
session
sbjs_current_add
Timestamp, referring URL, and entry page for your visitor’s current visit to your store
session
Marketing cookies are used to follow visitors to websites. The intention is to show ads that are relevant and engaging to the individual user.
OptinMonster is a powerful lead generation tool that helps businesses convert visitors into subscribers and customers.